

Palliative Care (PC) at its heart is a response to suffering that aims to comfort what we cannot cure. Suffering is universal, and in the end, all human beings are guaranteed the certainty of death. PC seeks to reduce or ease disease symptoms without necessarily removing the cause. Hospice care is a specific subset of PC, provided at the end of life (EOL) that aims to provide people with a calm, dignified, natural death. In 2002, the World Health Organization (WHO) declared palliative care a human right. In 2014, the World Health Assembly passed a resolution (WHA 67.9) that recognized the need to include palliative care as an integral component of universal health coverage. Thus, we all have a responsibility to ensure that PC is available and accessible to all of our people.
In 2002, the WHO defined PC as ”an approach that improves the quality of life of patients and their families facing the problems associated with life-threatening illness through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial, and spiritual.” This definition affirms the biopsychosocial-spiritual nature of what it means to be human.
The Caribbean region reflects the global trend of increasing rates of incurable non-communicable diseases (NCDs). These conditions often lead to unaddressed suffering when doctors focus on the numbers (blood pressure, sugar and cholesterol levels, and kidney function), the right drugs and medical intervention, and forget the human being whose suffering goes far beyond the medical issues. PC, which encompasses a compassionate, holistic approach to relieving suffering and improving quality of life at any stage of disease, would enable health care providers to better manage people with these NCDs. The “whole-person” framework better addresses the physical, psychological, social, and spiritual suffering associated with cancer as well as chronic diseases such as organ failure, emphysema, and dementia. The graphic below illustrates how PC and hospice care can be deployed.
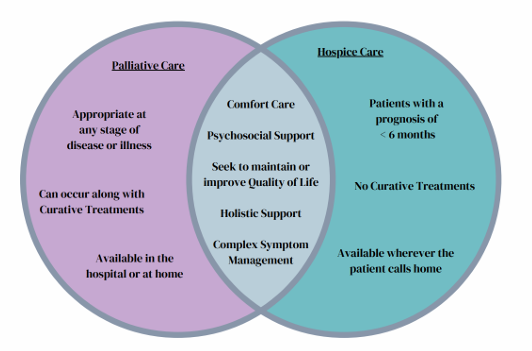
In the Caribbean, we are also seeing the shift to an aging population as birth rates decline and life expectancy increases. Yet we generally lack the medical awareness to diagnose and address EOL issues and the healthcare infrastructure to provide appropriate care for someone at that stage of life. It is not uncommon for people who are actively dying to be subjected to unnecessary medical interventions (e.g., tube feeding and intravenous fluids), resulting in avoidable suffering. Hospice or End-of-Life Care (EOLC) is a specific form of palliative care reserved for the final months of life (typically with a 6-month prognosis) and tailored to the needs of terminally ill patients and their families. It is usually an extension of existing palliative care services or can be initiated for terminally ill patients. A useful component of hospice care is Respite Care. This short-term inpatient stay provides primary family caregivers with a necessary break from their duties, thereby mitigating caregiver burnout. There is a profound need for this kind of care in the Caribbean.
A PC model that fits the needs of the Caribbean
Socio-economic and geographical factors contribute significantly to suffering in the Caribbean region. Lack of education, loss of income, transportation challenges, and housing that was never designed for people with mobility challenges more often cause greater suffering than the actual illness. This makes PC more of a community health issue than a strictly biomedical issue. But we also tend to have multi-generational households, communities where neighbors live in close proximity, and a tradition of informal caregiving provided at home. Faith-based and other volunteer service organizations tend to be actively involved in supporting community well-being. Our hospitals and government-run health care institutions are better suited to providing acute care, while chronic illness and aging require longer-term care that takes a whole-person approach and involves community engagement in care.
All of the above suggest that the Caribbean region would be better served by a PC model tailored to our needs and that leverages our strengths. In India, the Kerala region stands out for its success in delivering PC to those who most need it. The Kerala Model of Palliative Care (KMPC) is founded on a web of community linkages known as the Neighborhood Network in Palliative Care (NNPC). With its focus on primarily home-based care, sustained by community resources (human and material), and on strengthening the confidence and skills of local community members, KPMC is an example of a PC delivery option that could be adapted to the Caribbean context. A key defining feature is that community volunteers “own” and manage the service, while medical professionals and the government provide support. The links below provide more detailed information on this model.
Palliative care policy and practice in Kerala, India: Implications for Sustainable Development
Goal 3—Health and well-being – PMC- https://pmc.ncbi.nlm.nih.gov/articles/PMC12149619
The Kerala Model of Palliative Care: Social Capital and Sustainability — Transforming Care into
Communal Responsibility- IEC25266.pdf
What can we do to meet PC needs in the Caribbean?
The key components for effective PC delivery include good communication skills and a holistic approach to health. Although they are not specifically articulated and practised, these are also the foundations of good medical practice. Providing training and practice in communication skills and the management of common symptoms that respond well to a PC approach, as continuing education for health care providers already in the system, is one way to build PC capacity within existing primary care services. Ensuring that all undergraduate medical/nursing/allied health
care programs teach competency in basic PC, including EOLC, would increase awareness and improve the human resource capacity. Engaging local specialists, and collaborations with international institutions, can help provide this education.
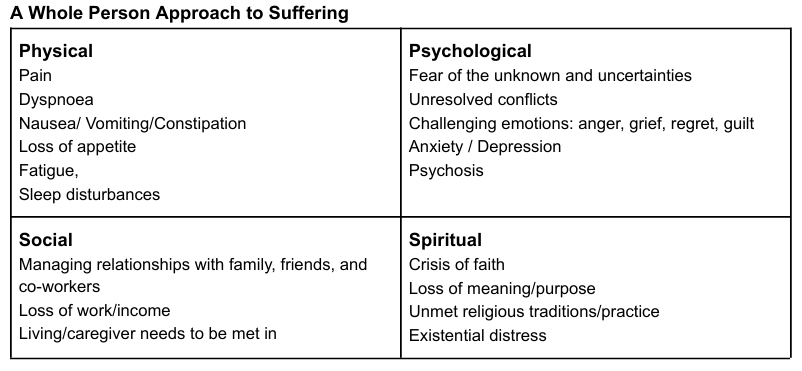
The sources of suffering based on the domains of personhood are summarised below. All undergraduate health care programs could adopt this assessment approach. Practising primary care providers can also be taught to assess patients using this framework
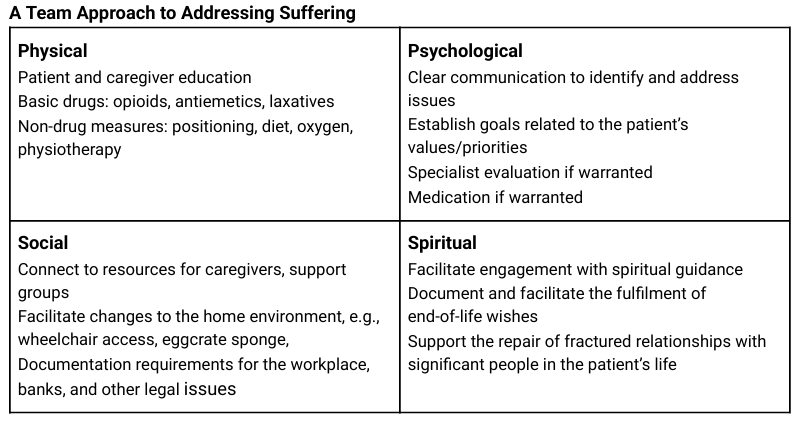
Once the total suffering has been identified, the following approach can help devise a holistic care plan that addresses all flagged domains. This requires seeing the whole human being rather than just the disease and a multidisciplinary team approach to care.
The “First World” models, founded on specialized infrastructure and funded by medical insurance, are not a good fit for our region. The Caribbean region’s health care landscape has its own challenges, including laws and policies that limit reliable and equitable access to basic medications such as opioids, and a shortage of PC specialists. We generally have a reasonably robust primary health care system. So, the better approach for us would be to embed PC within a system which already has the infrastructure to support it. Primary Care Physicians (PCPs) are essential in low-income societies, acting as the primary source of palliative care by managing pain, coordinating care, and facilitating home-based care to improve patient quality of life. They ensure continuity and comfort, reducing reliance on hospitals in under-resourced areas where specialty palliative care is scarce. Looking at suitable models like the KMPC for inspiration on how to establish our own PC delivery systems can be helpful.
Pooling the region’s resources, knowledge and experience, and collaborating, will allow us all to go further than if each territory travelled alone. To this end, the Palliative Care in the Caribbean – ECHO – PAHO/WHO | Pan American Health Organization is perhaps the longest-running and most widely subscribed resource supporting PC providers in the region. It consists of a monthly online meeting where a Caribbean practitioner presents a PC case for discussion for the first 40 minutes. This is followed by a didactic lecture from a PC specialist who is usually from a North American Institution. It is free to attend, and has also led to the formation of a Caribbean Palliative Care WhatsApp group where practitioners can reach out for advice or share information on PC matters. Over the years, the group has become a valuable source of knowledge and general support for PC providers in the region. The ECHO project is the result of a partnership between the Pan American Health Organization (PAHO), Massachusetts General Hospital, Jamaica Cancer Care and Research Institute (JACCRI) and Caribbean Palliative Care Association (CARIPALCA).
The Caribbean Palliative Care Association (CARIPALCA) is the regional umbrella organization, but it is currently dormant. Some territories have their own PC associations, as well as other organizations involved in PC activities. A range of PC services, both fee-based and free (NGO or government-funded), are provided in individual countries. Training and education are also available at various levels. The table below attempts to summarize these services.
PC offerings in the Caribbean
| Country | PC services/associations | Activities supported |
| Trinidad and Tobago | The Palliative Care Society of Trinidad and Tobago | Facebook (PCSTT) | Organize annual conferences/workshops for healthcare professionals and caregivers. Initiated the establishment of Caura – a PC unit. |
| Caura Palliative Care Unit – NCRHA– | 12-bed PC facility providing a range of services. NGO/government partnership. | |
| The Cancer Centre of Trinidad and Tobago – South | South-West Regional Health Authority-Cancer Centre of Trinidad and Tobago South Palliative Care Unit | Launched Feb 2025, 17-bed hybrid unit providing PC for cancer patients (EOLC, Respite care, Outpatient and some domiciliary care. | |
| About | LivHealthtt | Private health care provider with a focus on a range of PC services. Also, provide community PC training courses for professionals and informal caregivers | |
| Barbados | Barbados Association of Palliative Care on Strikingly | A registered charity organization partnering with the Ministry of Health and Queen Elizabeth Hospital. Provides bereavement counselling, and education/training for professionals and the general community. |
| Eden’s Way Clinic of Herbal Medicine | Facebook | Complementary care options in PC supporting the responsible use of herbal medicines | |
| Jamaica | Hope Institute- Hope Institute Hospital | Facebook | Government-funded cancer hospice providing outpatient PC for cancer patients. |
| Navigating Health Services- Home – Navigating Health Services | Private provider of cancer support, EOL planning, and lymphoedema therapy | |
| Holistic Harmony/ Dr Moina Spencer Ffrench moinaffrench@gmail.com | Private provider of specialist community-based PC + non-profit educational services for caregivers | |
| Consie Walters Hospice | Private provider: EOLC for cancer patients. | |
| University of the West Indies, Mona-all_programmes_for_2023-24_academic_year-_medical_sciences_3_0.pdf | Diploma in Geriatric Medicine offered through Mona Aging and Wellness Centre – for registered physicians | |
| Jamaica Cancer Care and Research Institute | JACCRI | Funding and support for PC training and education through seminars/workshops Support for experiential psilocybin retreats Research and publications on cancer care .jaccri.org/publications | |
| Cayman | Jasmine- Care – Jasmine | Free PC, hospice services, bereavement support -Funded primarily by the community (individuals and corporations) with donations of money, time, skills and other resources. |
| Belize | Belize Hospice Palliative Care Foundation (BHPCF)- Our Work | belize palliative care | A 20-year-old organization that provides free PC/hospice and EOLC Training for health care professionals and caregivers. Engages in patient advocacy. |
| Guyana | Beacon Foundation Ltd- beaconfoundationguyana.com | 40-year-old non-profit organization providing holistic care for patients with terminal illnesses and support for their families. Also, collaborate with other organizations to address suffering |
Myths about Palliative Care (PC)
Myth: It’s only given at the end of life as hospice care. PC is often equated with hospice care. While both PC and hospice care follow the same philosophy. PC is appropriate at any stage of a serious illness, while hospice care is only for EOL. Early integration of PC significantly improves quality of life by addressing issues like pain, fatigue, and anxiety, and decreasing unnecessary hospitalizations.
Myth: It means giving up hope. Provision of PC is associated with enhanced quality of life by changing focus to comfort, dignity and alignment with the patient’s values and priorities. A coordinated team approach addresses the physical, psychological, functional, and spiritual domains by engaging trained individuals, such as nurses, pharmacists, chaplains, social workers, physical therapists, and physicians, to execute comprehensive care plans that address the patient’s and family’s needs.
Myth: PC is only for pain. PC identifies and addresses a variety of physical, psychological, social and spiritual issues, such as fatigue, nausea, anxiety, depression, existential distress and loss of autonomy. Additionally PC includes bereavement care, grief counselling, and family support after a patient’s death.
Myth: It means losing independence. Early access to PC actually empowers patients and honours their autonomy by documenting their medical wishes (advance directives), clarifying, goals of care, and identifying trusted surrogates to make decisions if patients become unable to speak for themselves. PC also facilitates complex decisions regarding prognosis and treatment through clear communication to ensure that decisions are aligned with the patient’s values and wishes. PC ultimately ensures autonomy is protected when the patients are no longer able to
speak for themselves.
Myth: PC makes you die sooner. There is documented evidence (Early Palliative Care for Patients with Metastatic Non–Small-Cell Lung Cancer | New England Journal of Medicine) indicating that early inclusion of PC increases length of life as well as quality of life. By accepting that death is a part of life, and articulating what comfort means to the patient. PC helps to reduce useless medical interventions and focuses on achieving the comfort goals. The research and the lived experience affirms that this approach when applied early in the course of illness increases
quality and quantity of life.
Myth: PC makes you addicted to narcotics/morphine. Morphine is an essential drug for managing pain and shortness of breath in PC. When used according to established guidelines, morphine improves quality of life with very little risk of addiction. The common side effects of constipation and drowsiness can be managed and should not be seen as signs of addiction. Despite its effectiveness, research indicates that morphine remains underused for treating cancer-related pain across the Caribbean.









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}